
Person-centred care is a legal requirement for UK domiciliary care providers under Regulation 9 of the Health and Social Care Act 2008. It is also one of the most commonly cited areas of weakness in CQC inspection reports. This guide covers what person-centred care requires in practice, how the 2026 CQC framework changes affect how it is assessed, and what software features support providers in evidencing it.
Person-centred care isn’t a philosophy confined to policy documents. It is a measurable, auditable standard that CQC inspectors actively assess at every visit. Providers who treat it as a values statement rather than an operational practice find the gap between intent and evidence during inspection.
What Regulation 9 Requires From UK Care Providers
Regulation 9 of the Health and Social Care Act 2008 requires providers to deliver care that is appropriate to and meets the needs and preferences of each individual service user. That means care plans must reflect the person’s wishes, preferences, and goals.
Specifically, Regulation 9 requires that:
- Care and treatment is appropriate and reflects the needs and preferences of the service user
- Service users are involved in decisions about their care and have their views and wishes taken into account
- Care is provided with compassion and in a way that respects dignity
- The care plan is reviewed and updated when circumstances change
A care plan that was accurate at the point of initial assessment but hasn’t been reviewed when a service user’s health or preferences changed fails Regulation 9 regardless of how well care is delivered day to day.
How the 2026 CQC Framework Changes Affect Person-Centred Care Assessment
Under the new CQC framework currently in consultation for late 2026 implementation, person-centred care has moved from the Responsive key question to Caring. The five key questions, i.e., Safe, Effective, Caring, Responsive, and Well-Led, remain, but the 34 Quality Statements are being replaced by 24 Key Lines of Enquiry (KLOEs) with sector-specific rating characteristics for adult social care.
This shift means inspectors assessing person-centred care will do so through the lens of whether people are treated with compassion, dignity, and respect. The practical implication is that evidence of person-centred practice needs to come from care records, carer behaviour, and service user feedback simultaneously, not just from care plan documentation.
What inspectors look for under the Caring key question
- Care plans that reflect the individual’s stated preferences, communication needs, and cultural background
- Evidence that service users are involved in reviewing and updating their own care plans
- Visit records showing carers acted on individual preferences during the delivery of care
- Feedback from service users and families confirming they feel listened to and respected
- Preferred carer matching and continuity of carer records
What Person-Centred Care Plans Must Include Under NHS England Standards
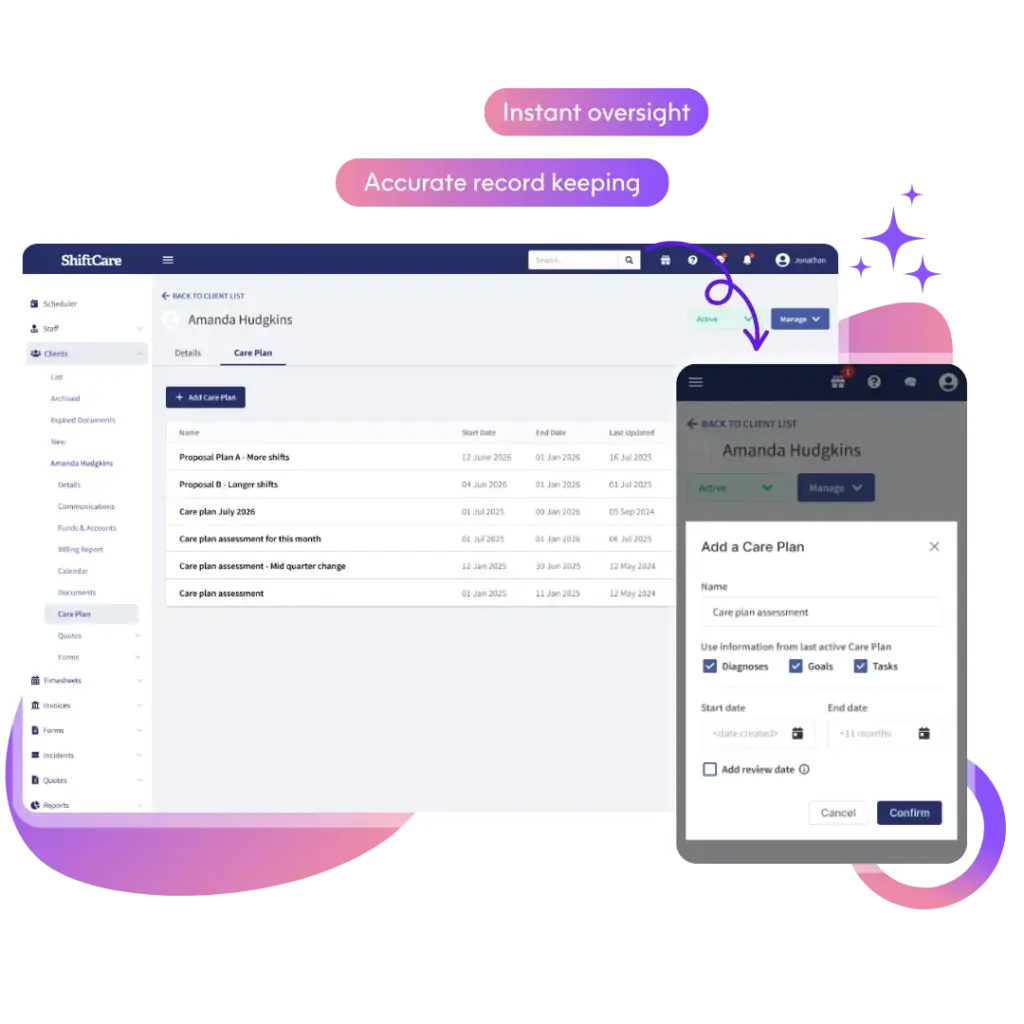
NHS England’s Digital Social Care Records (DSCR) framework sets 14 standards for how care records are captured, stored, and managed digitally. Person-centred care plans sit at the heart of those standards. A compliant digital care plan is not a list of tasks. It captures the person’s goals, preferences, history, and what matters to them in a way that any carer who hasn’t met them before can use to deliver personalised support.
Care plans built around scheduling logic tell inspectors that the visit happened. Care plans built around the individual tell inspectors how the visit was personalised. Under the SAF and the forthcoming KLOE framework, the second matters far more to a Caring or Good rating.
What a person-centred digital care plan should document
- The individual’s personal history, background, and what matters to them
- Communication preferences and any needs around language, literacy, or sensory impairment
- Goals and outcomes the person wants to achieve, not just support needs
- Preferences around routines, food, activities, and social engagement
- Advanced care planning documentation and Lasting Power of Attorney details where relevant
- Cultural, religious, and spiritual considerations
- Review dates and a record of who was involved in each review
How Continuity of Carer Supports Person-Centred Delivery in Practice
Person-centred care is harder to deliver when a different carer arrives at every visit. Skills for Care identifies continuity of carer as one of the most significant factors in service user satisfaction and safe care delivery. A carer who knows an individual’s preferences, communication style, and daily routine delivers more consistent, responsive care than one reading from a care plan for the first time.
CQC inspectors ask about continuity of carer directly under both the Caring and Safe key questions. Rostering decisions that consistently ignore preferred carer matching in favour of operational convenience create both a regulatory and a care quality risk.
Providers who embed preferred carer matching into scheduling decisions and document continuity of carer as part of their quality evidence build a demonstrable link between their rostering practice and person-centred outcomes.
What Happens When Person-Centred Evidence Gaps Appear at Inspection
If your software is built around scheduling as the primary data structure, the information it generates tells inspectors whether your care professionals arrived on time. It doesn’t tell them whether a service user’s nutritional intake has declined over six weeks, whether their personal goals are reflected in active care tasks, or whether their care plan was reviewed within the required timeframe. Those gaps are visible at inspection and carry real weight under the SAF.
Care plans that haven’t been reviewed to reflect changed needs, visit notes that describe tasks completed without any reference to individual preferences, and a lack of documented service user involvement in their own care planning are consistent findings in Requires Improvement reports under the Caring and Responsive key questions.
Build a Person-Centred Care Practice That Holds Up at Inspection
Person-centred care requires the right documentation structure, not just the right intentions. Care plans that capture what matters to the individual, visit records that evidence personalised delivery, and scheduling that supports continuity of carer all generate the evidence CQC inspectors expect to see across the Caring, Responsive, and Effective key questions.
ShiftCare’s care management platform supports person-centred care planning with structured digital care plans that capture individual goals, preferences, and communication needs. Rostering tools support preferred carer matching and continuity across visits, and care notes logged on mobile at the point of care create the timestamped visit evidence that links scheduling decisions to person-centred outcomes. The family portal keeps service users and their families involved in the care process between reviews.
Start your free trial today. See how ShiftCare helps UK domiciliary care providers build the person-centred evidence that CQC inspectors look for across every key question.


