
Medicaid claim denials cost home care agencies thousands of dollars every month. A claim gets rejected for missing documentation, an EVV mismatch, a coding error, or patient eligibility that changed without you knowing. Then it goes to appeal, which takes weeks or months. And sometimes you never recover the money at all.
Most agencies treat denials as billing problems, so they throw the issue back at the billing department. But that’s wrong. The root cause of most home care claim denials starts in operations, not in billing. It’s a visit that wasn’t logged correctly, a client whose insurance coverage wasn’t verified, or authorization data that didn’t sync. Your billing team is trying to process clean claims from dirty data. Fix the operational gaps and the downstream denials resolve themselves.
Step 1: Identify the Most Common Denial Drivers in Your Agency

Missing documentation ranks at the top of the list nationally. A claim gets submitted and rejected because the client’s physician didn’t sign the plan of care, visit notes are incomplete, or proof of medical necessity isn’t attached. Coding errors are a close second. EVV discrepancies cause denials too: the visit was logged on the schedule but not in the EVV system. Patient eligibility is another major driver: a client was eligible on the date of service but lost coverage by the time the claim was submitted. Authorization tracking failures make up the remainder: billing for visits when the client had already used up their authorized units.
Pull your denial reports for the last 90 days. Categorise every denial by type. This data will tell you exactly where your operational leaks are.
Step 2: Build Real-Time Visibility Into Your Data
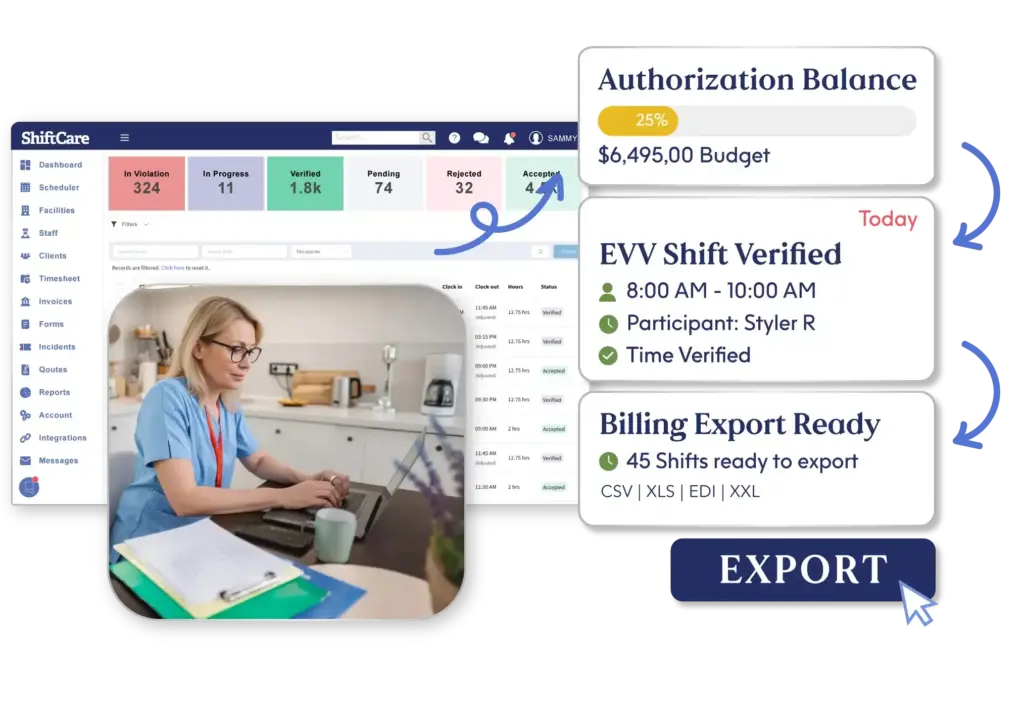
The first step in denial prevention is seeing what’s happening before it becomes a claim. Visit data needs to be captured at the time of service by your caregivers: start time, end time, service code, and notes. Patient eligibility should be verified before a visit happens, not after. Service authorizations need to be tracked actively, with alerts at 75% and 90% utilization. ShiftCare’s scheduling software and EVV module provide live visit capture, eligibility integration, and authorization tracking in a single platform.
Step 3: Fix the Operational Gaps, Not Just the Claims
Once you know your denial patterns, trace each one back to its operational cause. If you’re getting denials for missing physician signatures, the fix is a workflow that flags unsigned plans before claims are submitted, not a faster appeals process. If EVV mismatches are your primary denial driver, the fix is better caregiver training and a daily EVV audit, not better billing software. Address the upstream cause and the downstream denials resolve themselves.
Step 4: Integrate EVV and Billing
When EVV data and billing data don’t match, claims get denied. Make EVV the single source of truth for hours. When a caregiver completes a visit and logs it in your EVV system, that same data should flow into your billing system without manual re-entry. ShiftCare integrates scheduling, EVV, and billing so your caregivers log once and the data syncs everywhere.
Step 5: Run a Weekly Denial Prevention Audit
Every Friday, review the past week’s visits against your claim submissions. Are there visits not billed? EVV records that don’t match billing records? Fix mismatches immediately. This weekly habit catches the majority of denials before they happen.
Step 6: Track Denial Rate as an Operational Metric
Your denial rate is not a billing metric. It’s an operational health metric. Track it weekly, by denial type, by payer, and by caregiver team. If one group of caregivers produces a disproportionate share of EVV mismatches, that’s a training or management issue, not a billing issue. If denials spike after you onboard a new client, that’s an intake process issue. Metrics at this level of granularity point you to the right intervention rather than leaving you guessing.
Make Denial Prevention a Shared Responsibility
Your denial rate is not a billing metric. It’s an operational health metric. Track it weekly by denial type, by payer, and by caregiver team. If one group of caregivers produces a disproportionate share of EVV mismatches, that’s a training issue. If denials spike after you onboard a new client, that’s an intake process issue. Metrics at this level of granularity point you to the right intervention.
Train your caregivers quarterly on what good documentation looks like and what the consequences of incomplete records are. When denial prevention becomes a shared responsibility across your entire operation, the whole process gets tighter. ShiftCare integrates scheduling, EVV, and billing so caregivers log once and data syncs everywhere. Real-time authorization tracking, eligibility verification, and visit capture prevent denials before claims are submitted.
Start your free trial today! See how ShiftCare helps home care agencies reduce Medicaid claim denials.


