The Role of Documentation in Aged Care
Documentation serves several vital purposes in aged care, including:
- Enabling quality care by ensuring care workers are aware of patient information
- Facilitating effective communication between care providers
- Supporting you in meeting your legal requirements through providing records of services delivered, outcomes and/or any incidents
Documentation can be split into two types: core documentation and updates. Both enable care providers to deliver better quality services.
For your team members, documents are resources that let them know a client’s care needs, most recent health status and what to do if the client is unwell. These records function as a support, helping them improve health outcomes and respond to unexpected situations in a timely manner.
Examples of Documentation in Aged Care & How It Supports You
Aged care documentation includes:
Care plans provide your team with an overview of the patient’s needs and care expectations. Plus, they’re a helpful tool for you when reviewing services and extending contracts. A care plan should be updated at least once a year, with the client’s input.
- Strengths and needs assessments
A strengths and needs assessment should be completed before the care plan is drawn up, since it will inform you of what services an older person needs. During reviews, it can also help you measure the efficacy of the care provided.
- Risk assessments
Another document that should be completed before the care plan is created, a risk assessment serves as evidence that you have considered potential hazards and risks. Just like the care plan, it needs to be regularly updated and reviewed.
Progress notes both form a legal record of a client’s care and support your team in better understanding the client’s current condition and health. They can help you track developing health issues and progress alike.
Incident reports are vital records to complete after any concerning incident. They should detail what happened, the impact of the incident on the client and the actions taken to support them. These reports may be presented as evidence during inquiries.
How Home Care Electronic Documentation Can Support Your Team
Good documentation management systems are essential for all aged care providers, whether residential or at home. However, sharing information is of critical importance in home care, where workers cannot ask for support from on-site management.
Fortunately, electronic documentation and cloud-based storage allow home care workers to access all the information they need.
Modern Electronic Home Care Documentation
Electronic formats keep your documentation accurate, relevant and useful. It has been many years since pen-and-paper systems were the norm in the aged care industry.
However, some providers may find they are still reliant on outdated software that is slowing down their team, preventing smooth communication and having a negative impact on care recipients.
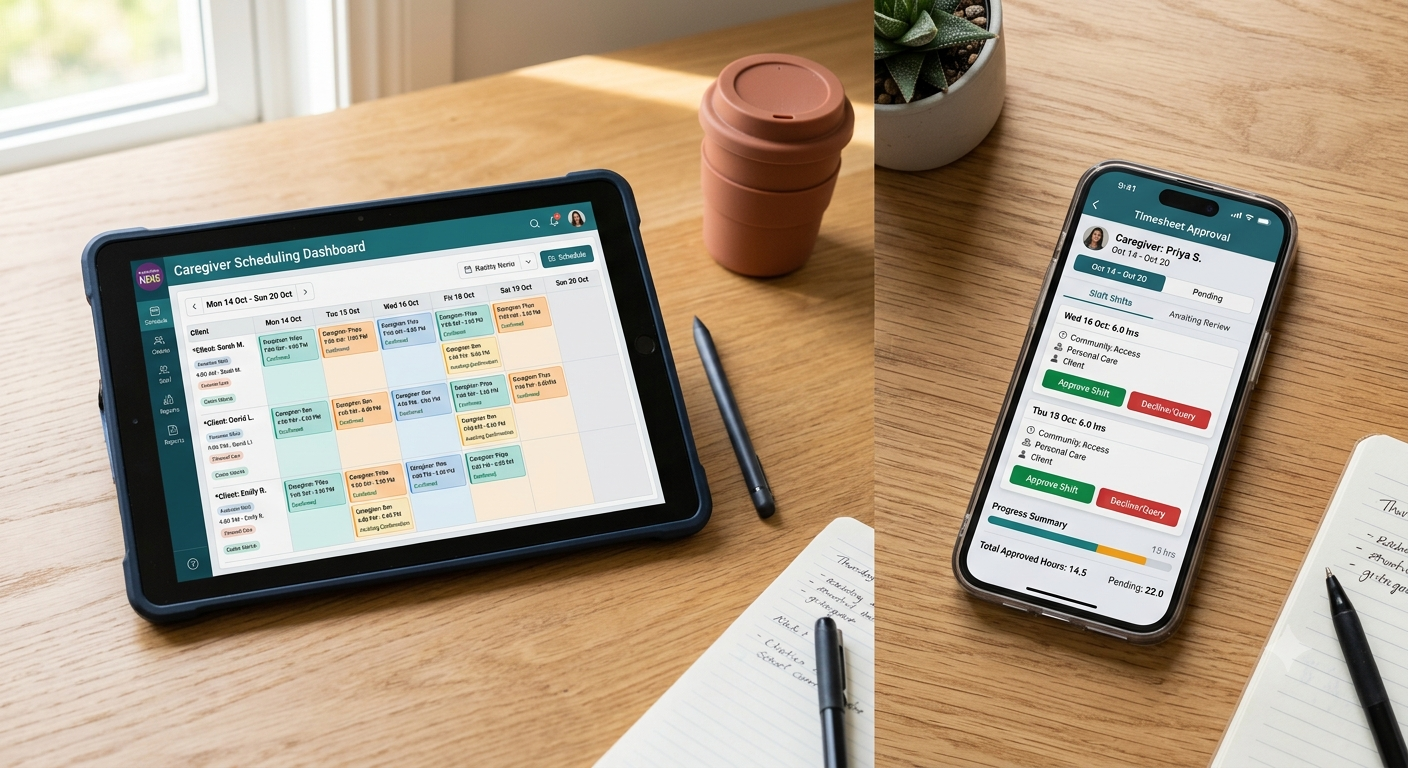
In modern care documentation solutions, your data should be stored in the cloud. This will allow for instant updates across all platforms, meaning that staff members can access accurate information on the go.
You should also be able to add records — such as progress notes — via mobile devices so that your team can report any incidents and add end-of-shift updates while the information is still fresh in their mind.
Security is also a key consideration. Your online records will contain private data that must be kept confidential. Outdated systems may not meet modern security requirements.
Read our blog Building Trust in the Digital Age: The Importance of Cybersecurity NDIS Software, to learn about the steps you can take to ensure you are keeping your information safe.
Effective Documentation in Residential Aged Care Facilities and Home Care: Best Practices
Client records should assist your team in providing excellent care and health service. To make sure they’re fulfilling this purpose, follow these guidelines:
Ensure Records Are Up to Date
Outdated information can present a risk to residents and at-home patients alike. Care plans and risk assessments must be regularly updated. Progress notes should be ordered chronologically, with the latest posts showing first.
Fortunately, modern solutions can help organisations stay on top of updating records. Check to see if your document management software includes document expiry dates and notifications.
Structure It Well and Cut the Fluff
Confusing, dense or poorly structured client information will be of limited use to your team. Make sure records are well-structured and concisely written so that team members can quickly find the information they need.
Custom templates can help you here by ensuring staff know exactly what to include in records. You may also find training them on documenting pays off.
Facilitate Access
Your team should be able to easily find and open the records they need. When faced with a health care emergency, they don’t have time to search through a complex filing system or open up the care plan on a computer. They need to quickly locate the relevant file on their mobile device and read it in seconds.
Electronic Documentation Made Simple
Effective documentation management ensures your team has the resources they need for quality care delivery. It also protects you by providing legal evidence and records of the care given.
Aged care providers like yourself have to stay on top of large amounts of paperwork. Ensuring that service records are high quality and core documents are up to date can be time-consuming. However, the right tools will mean that documentation is a helpful support, not a headache.
ShiftCare’s aged care software is designed to make electronic documentation management simple. Our secure cloud-based platform will ensure your workforce always has access to the information it needs. Record keeping is easy thanks to custom templates for progress notes, while expiry notifications will help you stay compliant with updated, accurate documentation.
To discover how electronic care documentation can simplify compliance and improve care quality, try ShiftCare for free.